“Doctor, will my face ever go back to the way it was before?” The question sounds simple, but for many people living with Systemic Sclerosis, it carries an ocean of fear, uncertainty, and silent emotional trauma. Scleroderma is often described medically as a chronic autoimmune disease characterized by skin thickening and fibrosis, but anyone who has spent time with these patients knows the disease extends far beyond the skin. It slowly changes appearance, confidence, relationships, daily activities, social interactions, and sometimes even a person’s sense of identity.
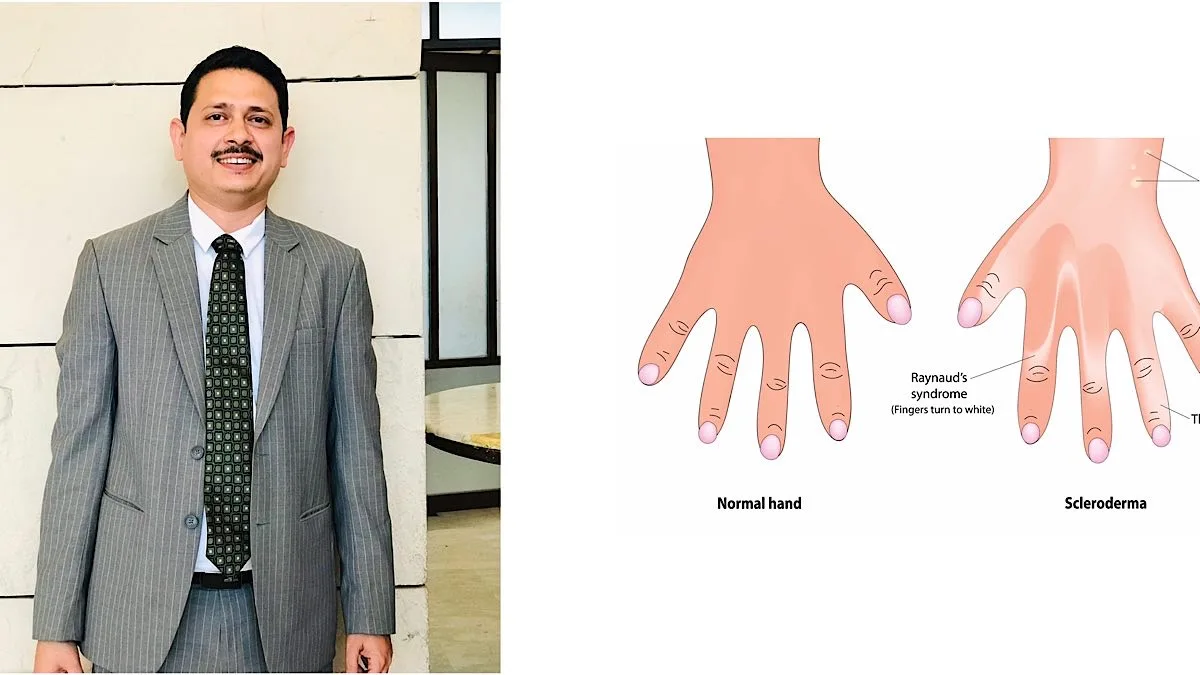
For many patients, the illness begins quietly. Fingers turning white or bluish in cold weather, mild stiffness of the hands, unexplained fatigue, persistent acidity, difficulty swallowing, tightening of facial skin, or breathlessness while climbing stairs are symptoms that are often ignored initially. But over time, the body starts changing in ways that are difficult to explain to others. The face becomes tighter, facial expressions reduce, the mouth opening becomes smaller, and the person standing before the mirror slowly feels unfamiliar to themselves. Clinically, we may call it “mask facies,” but behind that expressionless face lives a person constantly fighting thousands of emotions and questions.
Advertisement
The social impact of scleroderma is often immense yet poorly discussed. In a society where appearance unconsciously shapes perception, many patients become painfully aware of people staring at their altered face, tightened fingers, or skin changes. Some avoid social gatherings because they are tired of answering questions. Some stop taking photographs. Some hesitate to attend weddings or public functions. Young women frequently worry about marriage, relationships, motherhood, or whether they will be accepted by society. Many patients silently develop anxiety or depression, not because they are weak, but because chronic visible illness slowly erodes confidence. Unfortunately, emotional suffering often remains invisible behind laboratory reports and prescriptions.
Inside homes, the disease creates another layer of struggle. A mother may find it difficult to cook because finger tightening prevents proper grip. A teacher may struggle to hold chalk or write for long durations. A tailor may no longer handle fine stitching. A singer may notice voice changes due to reflux or lung involvement. Even simple daily activities like buttoning clothes, opening jars, brushing teeth, or eating comfortably can become challenging. Yet many patients continue managing households, careers, and families while carrying immense physical and emotional burdens that others rarely notice.
Medically, scleroderma remains one of the most complex autoimmune rheumatic diseases. The disease can affect not only the skin but also blood vessels, the lungs, the gastrointestinal tract, kidneys, joints, and the heart. Some patients predominantly suffer skin tightening, while others may develop serious lung fibrosis or pulmonary hypertension. Digital ulcers can make even touching objects painful. Severe reflux disease can affect nutrition and sleep. Breathlessness due to interstitial lung disease may silently progress for years before becoming obvious. This unpredictability itself creates fear, because patients constantly wonder what organ may be affected next.
One of the greatest challenges is delayed diagnosis. Early symptoms are often dismissed as “gastric problems,” “arthritis,” “winter allergy,” or “stress.” By the time proper rheumatological evaluation happens, organ involvement may already have progressed significantly. This is why awareness regarding autoimmune rheumatic diseases remains extremely important. Persistent Raynaud’s phenomenon, unexplained skin tightening, chronic reflux with hand symptoms, or breathlessness associated with autoimmune features should never be ignored.
Thankfully, modern rheumatology has significantly improved the outlook for patients with scleroderma. Advances in immunology, HRCT imaging, pulmonary function monitoring, vascular assessment, targeted immunosuppressive therapies, biologics, antifibrotic approaches, and pulmonary hypertension management have transformed care over the last decade. Today, management is not only focused on survival but also on preserving quality of life, maintaining independence, protecting organ function early, supporting mental health, and helping patients continue living meaningful and productive lives.
Perhaps the greatest lesson scleroderma teaches us is that illness cannot always be understood from outward expressions alone. Sometimes the least expressive face hides the deepest emotional battles. Behind every “mask facies” is a human being trying to preserve dignity, confidence, dreams, relationships, and hope. And perhaps that is where medicine becomes more than science, where listening, empathy, reassurance, and human connection become equally important as drugs and investigations.
The writer is a Consultant Rheumatologist and Academic Director of AIIR.